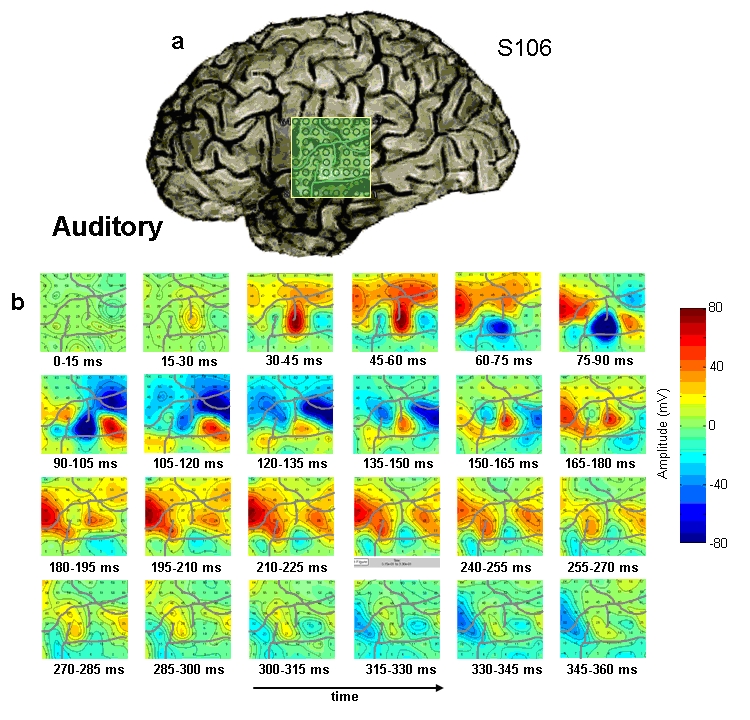
Example of intracranial ERP responses to an auditory speech stimulus recorded on a 8×8 macro-electrode grid
A core research area in our laboratory is the study of brain function in humans using subdural electrodes implanted inside the cranium. For purely clinical reasons, patients with epilepsy are sometimes implanted with such electrodes to localize their seizure onset prior to surgical therapy. This gives us the chance to study brain processes with unmatched temporal and spatial resolution, including recordings from single-units, without any additional risk to the patient. All our studies adhere to the strict ethical guidelines of the NYU School of Medicine guidelines for research involving human subjects and have current Institutional Review Board approval. Patient volunteers often enjoy participating in our sensory and cognitive experiments to alleviate some of the boredom an extended hospital visit can entail. Furthermore, patients see the value of our research and are often very interested in contributing to the advancement of scientific knowledge and medical treatments.
A clear advantage of ECoG over other neuroimaging methods is that it possess both high spatial (mm scale) and temporal (ms scales) resolution. The spatial resolution of iEEG varies depending on recording equipment. We are currently able to obtain both single and multi-unit recordings from extra-cellular laminar and Utah array microelectrodes and local filed potential recordings from surface strips and grids of electrodes, as well as depth electrodes (often placed in the hippocampus and amygdala). A further advantage of ECoG over MEG and scalp EEG is that intracranial recordings are not so susceptible to artifactual contamination from muscle movements and eye blinks, which regularly impair the quality of MEG and scalp EEG recordings, especially during language production.
One of the prerequisites of recording directly from the human brain is that the subject is a neurological patient who suffers from epilepsy. This raises the issue that the brain responses recorded from these patients may contain abnormal neuronal patterns and may not generalize to the general, healthy population. This possibility can never be ruled out, but steps can be taken to minimize its likelihood, such as recording from sites distant to the seizure focus and recording from patients with different etiologies, pathologies and anticonvulsant medications. Data contamination by interictal spiking is a prevalent problem and can be minimized by selecting testing periods where the subject is under anticonvulsive medication and by increasing the number of stimulus trials in case data have to be discarded. In many of our experiments we are also performing MEG and/or fMRI in healthy subjects and patients, allowing validation of the ECoG findings with other imaging methods in healthy subjects. One particular ECoG signal, the activity in the high gamma power (HGP) band (70-190 Hz, also called “broadband activity”), is of special interest to us since it possesses a high signal-to-noise ratio and is likely to reflect the aggregate spiking activity of neuronal populations immediately underneath the electrode and is thus directly related to increases and decreases in local neuronal activity.
You can find out more about the NYU ECoG Center at their web page: http://ecog.med.nyu.edu/